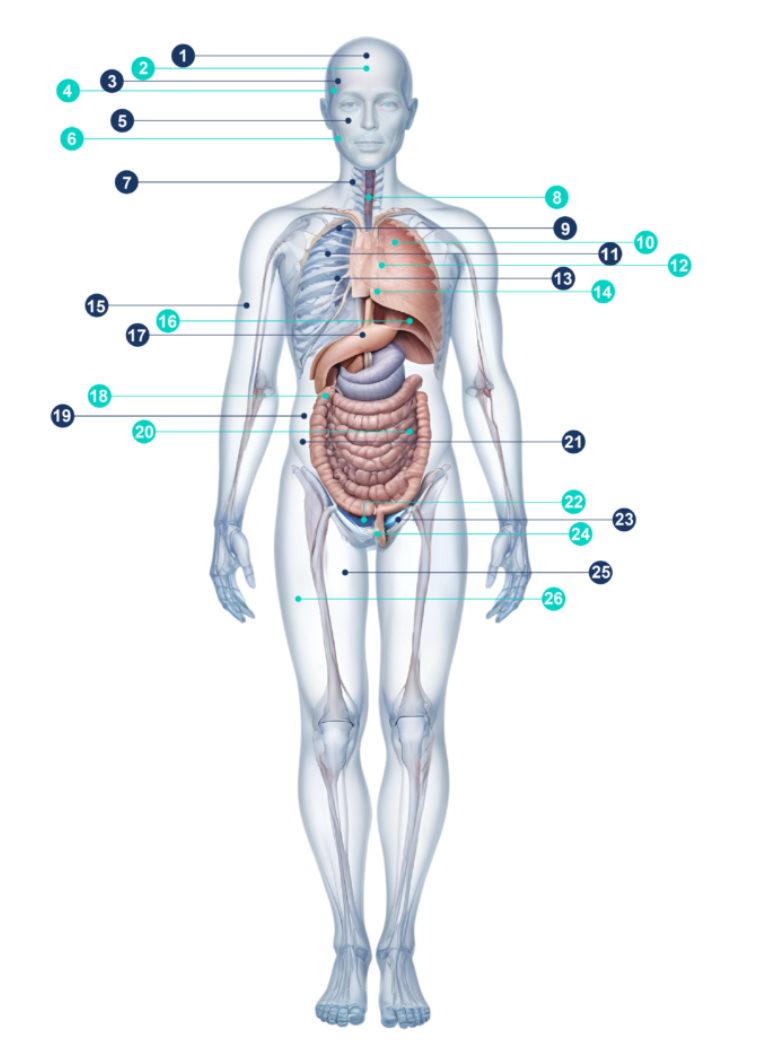
The Body Map
Discover yourself like never before with our Interactive Body Map. Explore key diseases we detect and the advanced scans we use. Click on the name of each Disease or Scan below to see detailed information about what is involved



Discover yourself like never before with our Interactive Body Map. Explore key diseases we detect and the advanced scans we use. Click on the name of each Disease or Scan below to see detailed information about what is involved
WhatsApp us
Dementia is not a specific disease, but rather is a descriptive term for a range of symptoms that are caused by a number of disorders that affect the brain. People with dementia have significantly impaired intellectual functions.
Vascular Dementia (or multi-infarct dementia “MID”) is caused by a series of mini strokes. MID is the second most common cause of dementia after Alzheimer’s disease in people over 65 and usually affects people in the age range 55 – 75, being more common in men than women.
A stroke is simply an interruption in, or blockage of, the blood supply to any part of the brain. If blood flow is prevented for any longer than just a few seconds, that part of the brain cannot get oxygen causing permanent damage.
We use MRI scanning to examine the blood vessels in the brain to spot early signs of narrowing and which left unchecked could lead to a blockage and a resultant infarct or stroke.
Cerebrovascular disease refers to a group of conditions and diseases that affect the blood supply to the brain. If a blockage prevents the brain cells from receiving oxygen, even for just a few seconds, permanent damage can result.
Cerebrovascular diseases include strokes or transient ischemic attacks (a ‘stroke’ which lasts less than 24 hours). There are 3 main causes:
We use MRI scanning to examine the blood vessels in the brain to spot early signs of narrowing and which left unchecked could lead to a blockage and Cerebrovascular disease.
An arteriovenous malformation (AVM) is an abnormal connection between arteries and veins that bypasses the usual method of connection, the capillary system. It can occur pretty much anywhere but is often observed in the Central Nervous System (usually as cerebral AVMs). The majority of people with an AVM are asymptomatic (i.e. they are carrying the disease or disorder but have not presented with any symptoms of the disease / disorder).
However, cerebral AVMs can present themselves in a number of different ways especially bleeding, severe headaches and a seizure or brain seizure. Bleeding from an AVM can be devastating and can cause severe, sometimes fatal, strokes.
A brain tumour, as with any other type of tumour, is a collection of cells, in this case in the brain, that are growing out of control. The normal life cycle of cells has become defective and they have carried on dividing causing a lump or tumour.
Tumours that start in the brain are called Primary Brain Tumours whereas those that have spread to the brain from elsewhere in the body are known as Secondary Brain Cancers or brain metastases.
There are more than 130 different types of brain tumours – either benign (non cancerous) or malignant (cancerous). Benign brain tumours generally grow slowly and are less likely to return after treatment and do not spread to other parts of the brain. Malignant tumours on the other hand grow faster plus there is a higher risk of them returning even after treatment.
Brain tumours are often named after the cell they develop from or the part of the brain they start in. More than half of all primary brain tumours are gliomas, developing from the supporting cells in the brain or spinal cord, the most common of which are astrocytomas. Early detection can have dramatically beneficial effects. The ability to detect and then treat for instance a low grade glioma before it progresses to become an advanced astrocytoma such as GBM (Glioblastoma Multiforme) can dramatically alter the prognosis and chance of cure.
Paranasal (i.e. near the nose) sinus and nasal cavity cancer is a disease in which malignant cancer cells form in the tissues of the paranasal sinuses and nasal cavity. Signs and symptoms can include, amongst others, sinus problems, headaches or pain in the sinus area, and frequent nosebleeds.
The most common type of paranasal sinus and nasal cavity cancer is squamous cell carcinoma though melanomas and sarcomas amongst others are also observed. Prognosis and treatment depends on where the tumour is located precisely and whether it has spread and of course the size of the tumour, the type of cancer, the patient’s age and general health.
Paranasal sinus and nasal cavity cancers have often spread by the time they are diagnosed and are hard to cure. After treatment, a lifetime of frequent follow up checks are essential because of the increased risk of developing a secondary cancer in head or neck. As with many of the conditions we can detect through an Echelon Health Preventative Health Assessment, early detection and prevention is more effective than cure
An acoustic neuroma is a type of brain tumour that develops from Schwann cells in the inner ear by wrapping around the vestibular (auditory) nerve. The vestibular nerve is responsible for carrying messages from the inner ear to the brain so is related to a person’s ability to hear as well as contributing to one’s sense of balance.
Almost all of these tumours are classified as grade 1 (slow growing) but although they are mainly benign, the symptoms tend to worsen over time. Symptoms are caused when the tumour grows to a point that it puts pressure on the acoustic nerve or those nerves nearby. Symptoms can include hearing loss (often on one side), tinnitus, fascial muscle weakness, headaches and dizziness amongst others.
Some acoustic neuromas grow so slowly that they can simply be monitored with regular scans and may not be treated. Others can grow more rapidly and require treatment either through surgery (where they can often be completely removed) or stereotactic radiotherapy (a highly targeted form of radiotherapy).
The carotid arteries are the main blood vessels supplying the brain. An atheroma or atherosclerotic plaque (‘ furring up’ ) is an accumulation of fatty material on the inner layer of the wall of the artery. The build up of these plaques makes the artery narrower (known as “stenosis”) and this process can alter blood flow making clots more likely to form.
The result of all of this is to restrict and occasionally prevent the supply of blood to part of the brain thus leading to a stroke. Alternatively, if an atheroma ruptures, it exposes the lining of the artery and a blood clot (thrombosis) forms over the damaged area. Fragments of these clots can then break off and go up to the brain, block a blood vessel and also cause a stroke.
Thyroid cancer develops from the tissues of the thyroid gland located in the front of the neck with symptoms including swelling or a lump. However, neck lumps are not uncommon and most are benign so careful examination and investigation by a skilled and experienced physician is important to avoid the risk of overdiagnosis of thyroid cancer.
Cancer of the thyroid is relatively rare, though the incidence is increasing. Notwithstanding that, if caught early, thyroid cancer (especially if the most common form – papillary) does have a high cure rate although almost all types of thyroid cancer are treatable using surgery.
As with all cancers, the growth of tumours in the lung is as a result of an abnormal / defective growth of cells outside of the normal cell life-cycle. Whilst there are many different types of lung cancer, the two main types are non small cell lung cancer (NSCLC), and small cell lung cancer (SCLC) which spreads more quickly and is often at a more advanced stage when diagnosed.
Anyone can develop lung cancer. Although the large majority of cases occur in people who smoke or used to smoke, the incidence of lung cancer in those who have never smoked is dramatically rising, for reasons which are not yet completely clear. In the UK, recent data shows that the proportion of non-smokers undergoing surgery for lung cancer jumped from 13% to 28% from 2008 to 2014. Amongst smokers, according to the British Lung Foundation, if you stop smoking, the risk does reduce over time. They say that after 10 years, your risk of lung cancer falls to half that of a smoker.
The real problem with diagnosing lung cancer is that often patients won’t have any symptoms of until the tumour becomes quite large. Often, the tumour is only discovered when the patient has an X ray or scan for a different reason, by which time the prognosis is frequently very poor.
Lung cancer still has the worst survival rates of all the major cancers with just 5% of people in the UK surviving 10 years plus. Yet CT scanning of the chest enables detection of cancers as small as just a few mm in size which greatly increases the chance of successful treatment to over 95% 10+ year survival.
An aortic aneurysm is a dilation (enlargement) of the aorta (the main artery in the body) that normally causes no symptoms except when ruptured. They are most commonly located in the abdominal aorta but can also be located in the thoracic aorta, close to where the artery leaves the heart.
The problem is that a ruptured aortic aneurysm almost invariably causes massive internal bleeding which is usually fatal. According to the NHS, around 8 out of 10 people with such a rupture either die before they reach hospital or do not survive surgery.
Aortic aneurysms occur in 4-12% of individuals (men much more commonly than women) but are usually small. They tend to grow slowly (around 1 – 2mm per annum) so early detection by means of a CT scan of the chest and/or abdomen allows any enlargement to be detected at an early stage and monitored for when prophylactic surgery would be most beneficial. A recent audit from the Royal College of Surgeons indicates that the success rate of such elective surgery is 98.6%.
Acute lung diseases generally refers to pneumonia (chest infection) which causes symptoms of cough with sputum, fever, and shortness of breath. It generally requires antibiotics to help it clear up but its location and extent is easily visible on a CT scan.
Other acute lung diseases include clots on the lung (pulmonary embolus), fluid on the lung (congestive cardiac failure), asthma and collapse of the lung (pneuomothorax), all of which can also be distinguished on CT scanning.
Pulmonary fibrosis is a lung disease which occurs when lung tissue becomes damaged and scarred. The thickened stiff tissue makes it more difficult for the lungs to work properly and as it worsens, it results in increasing shortness of breath.
There are many causes for pulmonary fibrosis, including long-term exposure to toxins and pollutants, radiation therapy, certain medical conditions and some medications. However, often the cause remains unknown.
While the lung damage caused by fibrosis cannot be repaired, medicines and therapies can sometimes help ease symptoms and improve quality of life. For some patients, a lung transplant is appropriate.
CT scanning is the most sensitive means of detecting pulmonary fibrosis at an early stage.
Chronic respiratory diseases affect the lungs and other parts of the respiratory system and generally develop slowly over many years but often getting worse with time. They may be caused by smoking tobacco or by breathing in secondhand tobacco smoke, chemical fumes, dust, or other forms of air pollution.
Types of chronic lung disease include asthma, chronic obstructive pulmonary disease (COPD), pulmonary fibrosis, asbestosis, and pneumonitis.
Over 370,000 people die each year in the UK from Coronary Heart Disease (CHD) – a condition in which fatty substances build up over the years inside the arteries of the heart. The build up (‘furring up’) of these fats (plaques) leads to a narrowing of the artery (stenosis) which can cause a progressive reduction in the supply of oxygen to the heart, especially when the heart is beating more quickly during exercise. Sometimes, these plaques rupture causing a blood clot to form on top of the affected area, which results in complete blockage i.e. a heart attack.
While CHD may lead to angina (pain in your chest) and breathlessness both of which can be precursors to a heart attack of some form, many patients do not get any symptoms or advanced warning of impending problems, and indeed CHD remains the commonest cause of sudden death in men over the age of 50. Further, approximately 1/3rd of individuals who suffer a heart attack have no risk factors.
However, modern CT scanning of the heart enables us to make an extremely accurate assessment of the earliest signs of CHD and thus to implement effective treatment strategies. The formation of plaques is usually accompanied by the deposition of calcium (chalk) within the plaque and this shows up extremely well on a CT scan. The so called coronary artery calcium (CAC) score provides an accurate and objective assessment of an individual’s overall risk of suffering a future heart attack, as opposed to a statistical risk based on population derived risk factors.
Occasionally the plaque does not calcify and the CAC score would be falsely reassuring. The ultimate assessment for the presence of CHD is the CT coronary angiogram which enables us to see directly inside the heart arteries and to detect plaque which has not calcified. This ‘soft’ plaque is the most vulnerable to causing a heart attack and is called ‘the widow maker’ being the most common cause of sudden death in otherwise fit and healthy middle aged men. One of the organisations Echelon Health works closely with analysed the detailed results of the CT Coronary Angiogram scans on 275 senior employees from a high profile and respected company a couple of years ago. The results demonstrated that for Coronary Artery Calcium scores, some 6.5% of the group had a score >400 which in some studies equates to a >20 fold increased risk of a heart attack.
Without screening, this would not have been identified, especially as none of these employees showed any symptoms. Worse still, the detailed CT angiogram images of the inside of the arteries of those same employees (utilising a resolution of just 0.3 mm) showed that:
Skin cancer is the out-of-control growth of abnormal cells in the epidermis, the outermost skin layer, caused by unrepaired DNA damage that triggers mutations. Mutations can cause skin cells to multiply rapidly and form malignant tumours. The main types of skin cancer are basal cell carcinoma(BCC), squamous cell carcinoma (SCC), melanoma and Merkel cell carcinoma (MCC). Melanoma skin cancer is the 5th most common cancer in the UK. Around 16,000 new cases of melanoma are diagnosed each year.
The two main causes of skin cancer are the sun’s harmful ultraviolet (UV) rays and the use of UV tanning machines. The good news is that if skin cancer is caught early, a dermatologist can often treat it with little or no scarring and a decent chance of eliminating it entirely. Often, skin cancer can be detected at a precancerous stage, before it has become a full-blown skin cancer or penetrated below the surface of the skin.
More than 1 in 4 skin cancer cases are diagnosed in people under 50, which is unusually early compared with most other types of cancer. Over recent years, skin cancer has become much more common in the UK. This is thought to be the result of increased exposure to intense sunlight while on holiday abroad.
If left untreated or detected at a late stage, melanoma can frequently spread to other parts of the body (metastasis), which makes curative treatment much less successful.
There are some 5,500 new cases of primary liver cancer in the UK each year with HCC (or hepatocellular carcinoma) being the most common form (around 90% of all cases). It is relatively rare in men and women aged under 45.
As with so many diseases and cancers, there are usually no early symptoms of liver cancer (with jaundice regularly being the first and only symptom of liver disease but reflecting advanced disease). Therefore, early detection provides the best opportunity for successful treatment.
The Gallbladder is a small sac located under the liver. It stores bile that is produced in the liver. Bile aids in the digestion of fats and is released as required into the small intestine.
Types of Gallbladder disease include inflammation, infection, stones or a blockage, as well as tumours. Gall stones typically occur in middle aged women and can be especially painful and debilitating. They can cause pain in the upper right abdomen that is severe but intermittent. If it results in infection there is associated marked fevers with nausea and vomiting and sometimes jaundice.
Gallstones are also a risk factor for development of gallbladder cancer. Detecting gall stones at an early stage can allow prophylactic removal of the gallbladder before they cause any serious problems.
The Adrenal glands are part of the endocrine system, a network of glands that produce and release hormones. Hormones keep an even balance of chemicals in the body helping us to respond and adapt to changing environmental circumstances. There are two adrenal glands, one on the top of each kidney, and they produce various hormones that are vital for the body’s functioning and survival.
Adrenal tumours are one of the most common tumours occurring in up to 6% of individuals. While most are benign, some are malignant and cancerous and are notoriously difficult to treat and cure, especially if they have grown to a large size and spread to adjacent tissues or other organs.
However, even benign looking adrenal tumours (‘adenomas’) need careful evaluation as they commonly secrete excess amounts of hormones which, while usually do not lead to overt symptoms, can cause long -term sub-clinical harm to the body.
A diverticulum is a small pouch emanating from the wall of the gut with multiple diverticulum being referred to as diverticulae – diverticular disease. They can develop in any part of the gut but are most prevalent in the colon (the large bowel). In general they do not cause symptoms unless they become inflamed or infected, resulting in inflammation and severe abdominal pain – diverticulitis. This can result in formation of an abscess or even perforation of the bowel.
Diverticular disease is easily detected by means of a CT virtual colonoscopy and if detected, preventive treatment involves a diet high in fibre, fruits and vegetables and restricting meat intake.
There is no evidence to support a link between diverticular disease and bowel cancer but if left untreated, diverticular disease can be extremely unpleasant. Diverticulitis is treated by antibiotics but surgery may be needed to drain an abscess or if a diverticulum bursts (peritonitis) and usually involves removal of the affected part of the colon. It may or may not involve a colostomy or ileostomy (intestine brought out through the abdominal wall to drain into a bag).
Healthy kidneys work to clean the blood by bringing ‘dirty’ blood into the kidney via the renal artery and with clean blood being taken back to the heart via the renal vein. As such they are the bodies main filtration system extracting water and waste in the form of urine which is then moved via the ureters to the bladder to be stored before being eventually expelled via the urethra.
Kidney (renal) tumours can be benign or malignant though kidney cancer is one of the more prevalent cancers occurring annually in the UK. 1 in 50 of us will develop renal cancer in their lifetime with it accounting for 4% of cancer diagnoses in men, being the 6th most common cancer. Over 12,000 people are diagnosed with it each year. However, with modern screening techniques, it is possible to detect these cancers at an early stage before they cause symptoms. If caught early, the chances of cure are much higher and often involves relatively straightforward keyhole surgery which preserves the function of the remaining normal kidney.
Other treatment options for small tumours include cryotherapy, high-intensity focused ultrasound or radio-frequency ablation.
Treatment depends on the type of bladder cancer, the stage of the diseases and the grade of the tumour so as ever, early detection is critical.
Bowel or Colorectal cancer (CRC) is the second most prevalent cancer that affects men and women with 1 in 14 men (7%) and 1 in 19 women (5%) being diagnosed with it in their lifetime. Around 268,000 people living in the UK today have been diagnosed with bowel cancer with over 90% occurring in people over the age of 50.
CRC occurs in the colon (the large intestine) or in the rectum with a roughly 80:20 split. The vast majority of these cancers develop from small polyps that are found on the bowel wall. The frequency of these polyps increases as we get older, occurring in approximately 10% of people over the age of 50. Most will never turn into cancer but over time, a minority do.
The good news is that these polyps tend to be slow growing on their path to becoming malignant (10 – 15 years) so if caught early, they can be removed long before they become a problem. But once they are malignant, the prognosis is poor and as with most cancers they can metastasise, spreading through the wall of the bowel into adjacent tissues or lymph nodes or via the blood stream to other organs, most often the liver.
Detected early, using screening techniques such as our non-invasive CT Virtual Colonoscopy, the prognosis is good. Left to the point where the polyps have become malignant and the resultant cancers causing symptoms, the prognosis is often poor with low chances of cure and palliative care being a likely course of action.
The prostate gland is usually the size and shape of a walnut and grows bigger as you get older. It sits underneath the bladder and surrounds the urethra, which is the tube that carries urine out of the body. The prostate’s main job is to help make semen – the fluid that carries sperm. The most common prostate problems are an enlarged prostate, prostatitis and prostate cancer.
While many prostate cancers grow slowly and probably do not affect mortality, as men die of other causes before the cancer causes significant issues, in others the cancer behaves more aggressively and indeed almost 12,000 men in the UK die from this disease each year.
Risk factors for developing prostate cancer include being male over the age of 50, a family history of prostate cancer and being black.
Most men with early prostate cancer don’t have any signs or symptoms but it can be detected by the combination of a blood test for a substance made by inflamed prostate tissue (Prostate Specific Antigen – PSA) and advanced MRI scanning of the prostate gland. While prostate cancer screening by the NHS is controversial and not routinely offered, we believe that men should have the option of knowing if they have prostate cancer and onwards referral to an experienced specialist to enable an informed decision to be made of all the treatment options including a watch and see policy if that is considered most appropriate.
Testicular cancer is relatively rare (accounting for approximately 1% of male cancers) though as with a number of other cancers, the incidence of it is on the rise for reasons that are still not fully understood. While there are several types of testicular cancer, the majority are so called germ cell cancers (seminoma and non-seminoma) similar to ovarian cancer in women. Although these can occur in men of all ages, it is perhaps unusual in tending to affect men under 50 more than over 50 and indeed it is the most common cancer in younger men.
For reasons that are unclear, white men have a higher risk of developing testicular cancer than men from other ethnic groups. Other risk factors include previous undescended testes, fertility issues, previous testicular cancer, calcium specks within your testes (micolithiasis) and a family history of testicular cancer.
Although aggressive if it develops, early detection and intervention is highly successful with around 95% of men surviving past 5 years. Treatment involves removal of the affected testis (occasionally both) although occasionally and in more advanced disease, additional chemotherapy treatment may be required.
Fortunately, screening for testicular cancer is straightforward with ultrasound scanning showing up any abnormalities very clearly.
Osteoporosis (brittle bones) is the condition by which bones lose their calcium and become weaker with increased risk of fracturing after relatively minor trauma. Once bones have been weakened by osteoporosis, signs and symptoms include:
In older people fractures such as that of the hip can lead to significant immobility and risk of further complications such as pneumonia or blood clots which themselves have a direct effect on mortality risk.
Losing bone is a normal part of ageing, but some people lose bone much faster than normal. Women also lose bone rapidly in the first few years after the menopause. Women are more at risk of osteoporosis than men, particularly if the menopause begins early (before the age of 45) or they’ve had their ovaries removed.
However, osteoporosis can also affect men, younger women and children. Many other factors can also increase the risk of developing osteoporosis, including:
The most common means of detecting osteoporosis is by means of a bone density scan. The NHS uses the DEXA scan but a more accurate technique is low dose CT scanning as this is the only means of measuring the true volume density of the middle of the vertebrae. Detection of osteoporosis at an early stage enables effective treatment to be commenced which slows or even reverses the loss of bone and reduces the risk of future fractures.
This extremely detailed scan looks directly at all the arteries and veins in your brain to assess whether there has been any narrowing or malformations of them. It also enables us to see tiny aneurysms (a bulging or ballooning in a weakened blood vessel wall).
Evidence of any of these could indicate a significantly increased risk of potentially catastrophic stroke or brain haemorrhage, although such early detection enables effective preventive treatment by modern radiology specialists.
We use a MRI Carotid Artery Angiogram (with the option of a CT Carotid Artery Angiogram in those who suffer from severe claustrophobia) to determine whether there is any narrowing of the neck arteries that supply blood to the brain. This would indicate an increased risk of stroke.
If any narrowing is considered severe enough, a procedure can be undertaken to ‘clear’ the blockage and reduce the risk.
In some assessments, we use Ultrasound as an alternative means of determining whether there is any narrowing of the neck arteries that supply blood to the brain. This would indicate an increased risk of stroke.
If any narrowing is considered severe enough, a procedure can be undertaken to ‘clear’ the blockage and reduce the risk.
An ultrasound of the thyroid performed by one of our Consultant Radiologists will look at the overall texture, blood flow and appearance of the thyroid gland.
Attention will be given to the presence of any cysts or nodules and their detailed characterisation which might indicate a possible malignancy.
With this scan we are looking for evidence of tiny nodules which could be the early signs of lung cancer. CT scanning is the most sensitive means of detecting lung cancers and with our experienced specialist chest radiologists, we have detected cancers as small as 1-2 mm.
It is far more sensitive than X-rays which can generally only detect tumours of 10mm in size, and MRI scanning which just cannot accurately image the chest at all.
The CT scan will also show up any areas of fibrosis or previous asbestos exposure, as well as signs of chronic infection and bronchiectasis.
Our scan of your heart is divided into two main elements. The first, a CT Heart Scan (Calcium Score) examines your overall heart arteries for any calcium deposition. As calcium is only deposited during the process of atheroma (commonly known as ‘furring up’ of the arteries), measurement of the total amount of calcium in all the heart arteries provides the most accurate assessment of the overall extent of atheroma. Numerous long-term prospective medical studies, involving hundreds of thousands of patients, have shown this to be a very accurate assessment of the overall risk of a future heart attack. Its great advantage is that it distils all of the risk factors and genetic predisposition into an objective and quantifiable risk.
This is the second part of our Heart Scan and is a more advanced scan that involves injection of dye into a vein in the arm and which then allows direct visualisation of the inside of your heart arteries.
This determines the exact location and severity of any atheroma; people with significant stenosis of one or more of the heart arteries have a very high chance sooner or later of having a heart attack, but which can be prevented by insertion of a stent.
The CT angiogram is unique in its ability to also visualise the so called ‘soft plaque’ which is atheroma that has not yet calcified and which is the most vulnerable to rupturing and causing a heart attack.
This is the so called ‘widow maker’ lesion which cannot be visualised by any other means but is one of the most common causes of sudden death. It classically affects individuals who have few if any risk factors for heart disease and who appear, superficially at least, to be fit and healthy.
We have specially selected The Mole Clinic, an award-winning, dermatologist-led skin lesion clinic to carry out a Full Body Mole Screen for us. Established in 2003, The Mole Clinic leads the UK in skin cancer screening and mole removal (for biopsy & cosmetic reasons). Their specialist nurses and GPs, consultant dermatologists and plastic surgeons deliver high quality clinical care to 40,000 patients every year.
Depending on the package you select from Echelon Health, a specialist nurse from the Mole Clinic will come to our Clinic at 68 Harley Street on the day of your Health Assessment and carry out a Full Body Mole Screen with the objective of identifying any visually atypical moles.
If the nurse considers it appropriate, she will also offer you the opportunity to have one or more Single Mole Scans undertaken on a visually abnormal or new or changing mole. A dermatoscope and a digital camera will be used to record an image 1 – 2 mm beneath the surface of the mole. The image is remotely assessed by a specialist skin doctor, the results of which will be discussed with you by your Echelon Health Physician when you come for the follow up consultation for your Echelon Health Assessment.
An Electrocardiogram (or ECG) is an important test that records the rhythm, rate and electrical activity of your heart. It is completely painless and takes only a few minutes.
ECG traces from healthy hearts have a characteristic shape. If the ECG shows a different shape of ‘trace’ it provides us with a first indicator of a potential problem with your heart, as well as determining any rhythm abnormalities
The CT scan of the abdomen looks at all the organs within the abdomen including:
This scan also visualises the rest of the aorta for any abdominal aneurysm.
This scan is looking for colonic polyps and early indications of possible cancer. Almost all colon cancers develop over a period of 10 – 15 years from tiny polyps which gradually increase in size and eventually turn into a cancer.
As with all cancers, waiting until the cancer causes symptoms such as weight loss, bleeding, or obstruction to the colon means that it is likely to have already spread and cure is frequently impossible.
However, this long process of conversion means that almost all colon cancers are preventable by undergoing an effective means of screening (such as with a CT virtual colonoscopy) for the polyps and if one is found, then removing it.
The 3T (Tesla) MRI scan of your prostate combined with the PSA blood test, is the most accurate means of screening for prostate cancer.
It is far superior to the PSA blood test alone or rectal ultrasound scan and by accurately imaging all of the different parts of the prostate gland provides a detailed assessment of any abnormalities.
One in eight men in the UK will get prostate cancer, mainly affecting men over 50 and with increased risk if there is a family history.
The testicular ultrasound uses sound waves to create images of the scrotal contents – testes, epididymis, arteries and veins supplying blood to the testes. It looks for any evidence of:
A CT Bone Density scan is an extremely accurate method of measuring the density of your bones and determining the presence of osteoporosis and risk of future bone fracture in your spine and hip.
It is more accurate than the traditional (dual energy x-ray adsorption) DEXA scan as it provides a true measurement of volume density (mg/cm3) of the spine vertebrae and is not subject to external influences such as calcified lymph nodes or calcium in the aortic.
Breast Cancer is the most common cancer in the UK population, representing around 15% of all new cancer cases. A woman born after 1960 and living in the UK has a 1 in 7 lifetime risk of developing breast cancer (the risk for men is 1 in 870).
There is no one cause of breast cancer. Some risk factors are inherited and some are incurred throughout one’s life. Others are present in the environment, although modern life would appear to be increasing the risk of developing breast cancer.
The best and most reliable method of detecting early breast cancer is to use a Digital Mammogram. These deliver very low levels of ionizing radiation which the NHS estimates increases the risk of breast cancer to be 3 – 6 cancers per 10,000 women who are screened every 3 years from 47 to 73. Given that the lifetime risk of developing breast cancer is 1 in 7 it can be seen that the risk of digital mammogram is extremely small compared to the likelihood of early detection.
The digital mammograms have significant advantages over the traditional film mammograms in not only emitting lower radiation but being more sensitive, especially in women with dense breasts and peri-menopausal.
The spleen is located under your rib cage in the upper left part of your abdomen. It is part of the lymph and immune system and works as a drainage system helping protect the body against infection.
White blood cells produced in the spleen surround bacteria, dead tissue and foreign matter as the blood passes through the spleen as well as filter blood in general, removing abnormal blood cells from your bloodstream.
An enlarged spleen is not always a sign of a major problem (it could be going through a period of hyperactivity) but it can be caused by infections and cancers, such as Leukaemia or Lymphoma.
The ovaries are two small glands that make up part of the female reproduction system having two main functions; production and storage of eggs, and the production of the female sex hormones, oestrogen and progesterone.
There are three types of Ovarian cancer with epithelial cancer tumours comprising around 90% of all ovarian cancers. These tumours occur most commonly in women between the ages of 40 and 60.
Ovarian cancer is the sixth most common cancer in women in the UK, with around 7,300 women diagnosed every year. Symptoms of advanced ovarian cancer include:
The prognosis for ovarian cancer depends on the stage of your cancer and the extent to which it has metastasized. Again, early detection is critical as this results in a 5 year survival of over 94%. Unfortunately currently in the UK only about 20% of ovarian cancers are found at an early stage. There is no NHS screening program for this disease despite recent trials demonstrating the effectiveness of the combination of blood tests for a specific ovarian cancer marker together with imaging of the ovaries by ultrasound scanning.
The (full field) digital mammogram uses the same x-ray technology as conventional mammograms, but instead of using film, solid-state detectors are used to record the x-ray pattern passing through the breast. These detectors convert the x-rays that pass through them into electronic signals that are sent to a computer. These digital images can be lightened or darkened, and certain sections can be enlarged and looked at more closely. In general, this makes digital mammography the most advanced and sensitive means of assessing the breasts for possible cancers, especially in dense breasts.
The pelvic ultrasound scan uses sound waves to create images of the female pelvic organs – ovaries, cervix, fallopian tubes and uterus.
It is used to measure and evaluate the size, shape, and position of the uterus and ovaries